Which Antibacterial Agent Performs Best for the Treatment and Clearance of Chlamydophila Felis Infection in Cats?
a Knowledge Summary by
David Mills MA, VetMB, CertAVP(VC), MRCVS1*
1RSPCA Putney Animal Hospital, 6 Clarendon Drive, London, SW15 1AA
*Corresponding Author (dmills@rvc.ac.uk)
Vol 2, Issue 1 (2017)
Published: 07 March 2017
Reviewed by: Eva Spada (DVM, PhD) and Kit Sturgess (MA VetMB PhD CertVR DSAM CertVC FRCVS)
Next Review date: 20 March 2019
DOI: 10.18849/VE.V2I1.55
Clinical bottom line
Based on the current evidence, oral doxycycline (10mg/kg PO q24h or 5mg/kg PO q12h) for at least 21 days represents the most efficacious treatment, both in terms of clinical improvement and permanent clearance of Chlamydophila felis infection in cats. In chronic infections, or where the duration of disease is unknown, a longer treatment course of 28 days is indicated. There is limited evidence that co-amoxiclav (12.5-22.5mg/kg q12h PO) may be used as an alternative, though a treatment period of at least 30 days is required.
Question
In feline patients infected with Chlamydophila felis (C felis), which antibacterial regime shows greatest efficacy in both improving clinical signs and permanent clearance of the organism?
The evidence
Whilst the methodology of most of the available studies is reasonable, their usefulness is limited due to most being experimental trials, and all having low numbers of participants. The use of experimental animals with defined infection periods limits extrapolation to general practice where the chronicity of infection is unknown, especially in stray or shelter cats. Feline chlamydophilosis has attracted a reasonable amount of research interest, and various antibacterial regimes have been trialled: doxycycline, co-amoxiclavpotentiated amoxicillin, enrofloxacin, pradofloxacin, azithromycin, roxithromycin, as well as topical fusidic acid and chlortetracycline. In the case of potentiated amoxicillinco-amoxiclav enrofloxacin and pradofloxacin, these trials were funded by manufacturers of veterinary-licensed versions of these compounds. Nevertheless, from the studies available, systemic doxycycline has shown repeated and significant superiority to other antibiotics in both treating the disease and preventing recrudescence, if a course of sufficient length is administered.
Summary of the evidence
Sykes (1999)
| Population: |
Experimental colony cats aged 10-12 months weighing approximately 5kg. |
| Sample size: |
8 cats (3 neutered males, 5 entire females). |
| Intervention details: |
- All cats pre-infected with feline herpes virus 3 months pre-trial and asymptomatic.
- All cats infected with cultured C. psittaci via cornea and after 6 days split into one of three treatment groups:
- 4 cats treated with doxycycline 5mg/kg PO q12h for 21 days.
- 4 cats left untreated.
- Monitoring of response to treatment:
- PCR and culture from conjunctival swabs daily (objective).
- Clinical signs of infection (non-blinded except for day 9 when an outside clinician blinded to treatment groups used).
- Separate rooms for each group.
- All treated cats euthanised on day 41, all untreated on day 64, and tissue submitted for chlamydial DNA PCR analysis.
|
| Study design: |
Non-randomised, non-blinded controlled trial. |
| Outcome Studied: |
- Comparison of PCR versus culture in diagnosis.
- Investigate whether shorter course of doxycycline for 28-42 days is sufficient to clear infection with C psittaci.
- Investigate possible sites of persistent infections following conjunctival clearance.
|
Main Findings
(relevant to PICO question): |
- Doxycycline-treated cats:
- Rapid improvement in clinical signs, average duration of signs 9.3 days.
- PCR negative after 8 days on average.
- Remained PCR/culture negative and disease free following treatment end until euthanasia on day 42.
Untreated cats showed signs for 30 days on average, PCR positive for 30.5 days on average. |
| Limitations: |
- Insufficient numbers to answer all three questions.
- Very small study numbers (4 treated cats) which preclude the strong conclusion that 21 days of doxycycline is sufficient.
- Short follow-up of 14 days post-treatment cessation.
- Clinical signs reported in untreated groups correlate poorly with natural infections, with cats in the study developing a severe rhinitis. This suggests a particularly virulent experimental strain and the study does not detail whether the inoculum was a field or experimental isolate. Limits extrapolation to field cases.
- Use of experimental colony cats limits extrapolation to field or natural infection. This represented a mono-infection, compared to field infections, where multiple infections, infectious dose, strain variation, genetic diversity of the cats and nutritional plane could impact on severity of infection and response to treatment.
- Only a single blinding event at day 9 with an outside clinician – rest of clinical sign logging was by unblinded investigators.
- Questionable use of an untreated group – these cats lost weight, had reduced appetite and generally suffered for an extended period with the disease. The authors’ aims regarding treatment were to ascertain a shorter course of doxycycline so different treatment length groups could have been used.
|
Sparkes (1999)
| Population: |
Pathogen-free experimental colony cats aged 4-11 months. |
| Sample size: |
24 (21 entire females, 3 neutered males). |
| Intervention details: |
- Inoculated with field strain of C. psittaci via cornea
- 7 days post-infection randomised into 4 treatment groups (6 cats in each):
- Placebo (topical artificial tears)
- Topical 1% chlortetracycline drops to both eyes q12h
- Topical 1% fusidic acid drops to both eyes q12h
- Doxycycline 10mg/kg PO q24h & topical 1% fusidic acid drops to both eyes.
- All treated for 28 days.
- Monitoring of response to treatment:
- Culture from conjunctival swabs to generate chlamydial isolation scores (objective)
- Clinical signs recorded at same time (subjective)
- Separate rooms not available so randomly assigned to one of three rooms during trial.
|
| Study design: |
Randomised, non-blinded controlled trial. |
| Outcome Studied: |
Comparison of topical and systemic therapies for the treatment of experimental chlamydiosis. |
Main Findings
(relevant to PICO question): |
- Doxycycline/fusidic acid group:
- Significantly fewer clinical signs (p<0.011) from day 1, maintained throughout with the exception of day 9.
- Culture negative from day 4 post-treatment commencement and throughout the study thereafter (except 1 cat on day 18)
- Significantly (p<0.05) lower median duration of shedding (3 days) than placebo and fusidic acid groups (28 days).
- Chlortetracycline group:
- Lower median shedding duration (8 days) than placebo and fusidic acid groups (28 days)
- Higher median shedding than doxycycline/fusidic acid group (3 days)
- Most cats in placebo and fusidic acid only groups were still shedding at the end of the study.
- Fusidic acid had no treatment effect above placebo for chlamydophilosis.
|
| Limitations: |
- Small numbers of cats in each treatment group.
- Randomisation method for assigning treatment groups and room to be housed is not detailed.
- Use of experimental colony cats limits extrapolation to field or natural infection. This represented a mono-infection, compared to field infections, where multiple infections, infectious dose, strain variation, genetic diversity of the cats and nutritional plane could impact on severity of infection and response to treatment.
- Housing cats together from different treatment groups was a confounder that was not controlled for, and may have led to false positives from cross-contamination e.g. cat from doxycycline/fusidic acid group on day 18.
- Use of clinical scoring is subject to subjective bias, especially as the treatment groups were not blinded to the investigators.
- Culture of chlamydial organisms is less sensitive for detecting chlamydial organisms than PCR, but has the advantage of only identifying live bacteria.
- No long-term follow-up, so the persistence of freedom from infection in the doxycycline/fusidic acid and chlortetracycline groups could not be assessed.
- Funded in part by producers of fusidic acid eye ointment at that time (Leo Laboratories) – theoretically fusidic acid (working on primarily gram-positive organisms) would have no effect on gram-negative chlamydial organisms.
|
Sturgess (2001)
| Population: |
Pathogen-free experimental colony cats aged 5 months. |
| Sample size: |
24 (13 females, 11 males). |
| Intervention details: |
- Inoculated with a field strain of C. psittaci via the cornea.
- 7 days post-infection randomised into 3 treatment groups (8 cats in each group):
- Placebo (gelatin capsule)
- Doxycycline 10-15mg/kg PO q24h
- Co-amoxiclav 12.5-22.5mg/kg PO at 0900 and 1700
- All treated for 19 days.
- Placebo group treated with co-amoxiclav for 30 days after trial end as a model of chronic infection.
- Co-amoxiclav group were treated with further 30-day course co-amoxiclav after infection returned after 14-20 days.
- Monitoring of response to treatment:
- Culture from conjunctival swabs taken three times a week (objective) to generate a chlamydial isolation score.
- Clinical scoring of disease (subjective but investigator blinded to treatment group) including weight and rectal temperatures (objective).
- Trial formally concluded after 91 days and cats observed daily for 6 months after this.
|
| Study design: |
Randomised, single-blinded controlled trial. |
| Outcome Studied: |
Comparison of systemic co-amoxiclav with doxycycline and an untreated control group in the treatment and clearance of C psittaci infection in experimentally infected cats. |
Main Findings
(relevant to PICO question): |
- Doxycycline and co-amoxiclav groups versus placebo:
- Isolation scores significantly lower by day 9 (p<0.01)
- Fivefold decrease in clinical scores in first week (p<0.01)
- Doxycycline group showed no recurrence after treatment end, demonstrating efficacy in clearing acute infections.
- Co-amoxiclav showed efficacy in acute infections, but with high rate of recurrence (62.5%) between 14-20 days after treatment end.
- Co-amoxiclav given for 30 days in chronic disease model cats (formerly placebo) and recurrent cats (following initial 19 days treatment) cleared infection with no recurrence.
|
| Limitations: |
- Small number of participants per treatment group (8) make statistical tests less valid, especially with no confidence intervals stated.
- Randomisation method for assigning treatment groups not detailed.
- Use of experimental colony cats limits extrapolation to field or natural infection. This represented a mono-infection, compared to field infections, where multiple infections, infectious dose, strain variation, genetic diversity of the cats and nutritional plane could impact on severity of infection and response to treatment.
- Culture is less sensitive than PCR for the detection of chlamydial organisms – the 5 cats from the co-amoxiclav treated group that showed recrudescence were likely still infected by the end of treatment, which was not detected by culture.
- Clinical scoring is subject to subjective bias, though this was reduced by blinding the investigator to the treatment group.
- Author conclusions describe co-amoxiclav as an effective treatment in acute and chronic stages of chlamydiosis, but with the proviso that a further 30 day treatment course may be required after treatment of acute phase. This would mean a 49 day treatment course versus 19 days for doxycycline.
- Co-amoxiclav is a time-dependent antibiotic, so treating at 0900 and 1700 is likely suboptimal in maintaining MIC values in conjunctivae for sufficient periods.
- No investigation into the effects of doxycycline in chronic chlamydophilosis.
- Funded by Pfizer Animal Health, manufacturers of a licensed co-amoxiclav preparation for cats.
|
Owen (2003)
| Population: |
Pathogen-free experimental colony cats aged 5-6 months. |
| Sample size: |
9 (3 entire females, 6 neutered males). |
| Intervention details: |
- Inoculated with field strain of C felis via the cornea
- 4 days post-infection all cats were showing clinical signs and randomly assigned to one of 3 groups:
- 2 cats untreated.
- 2 cats doxycycline 10-15mg/kg PO q24h.
- 5 cats azithromycin 10-15mg/kg PO q24h for 3 days then twice weekly.
- Treatment for 28 days.
- After initial treatment period the 2 untreated cats were given azithromycin 10-15mg/kg PO q24 for 25 days as a model of chronic disease.
- At the end of the trial the 2 initially untreated cats and 5 azithromycin cats were given a 28-day course of doxycycline to eradicate infection.
- Monitoring of response to treatment:
- Culture from conjunctival swabs (objective).
- Clinical scoring of disease (subjective, but investigator blinded to treatment group).
- Cats housed in 2 rooms, with one cat from the untreated group and one from doxycycline group in each room and the rest from azithromycin group.
- Monitored for 6 months post-trial for recurrence.
|
| Study design: |
Randomised, single-blinded controlled trial. |
| Outcome Studied: |
Determination of the efficacy of azithromycin compared to doxycycline-treated controls for the treatment of C felis infection in experimentally infected cats. |
Main Findings
(relevant to PICO question): |
- Doxycycline group:
- Culture negative 7 days after starting treatment.
- Rapid decrease in clinical scores from day 2.
- No recurrence after initial treatment course.
- Cleared infection in chronically infected cats (5 azithromycin group cats and 2 untreated cats) at end of study with 28-day course.
- Azithromycin group:
- Culture negative 7 days after starting treatment.
- Rapid drops in clinical scoring from day 2.
- Infection cleared in only 1 out of 5 cats (20%). Rest either remained positive or became positive again whilst still on treatment or after treatment end.
- Azithromycin failed to clear chronic infection in the two untreated cats given azithromycin daily for 25 days.
|
| Limitations: |
- Small numbers precluded statistical analysis.
- Randomisation method for assigning treatment groups and housing not detailed.
- Experimental colony cats, due to their husbandry, may possess a less robust immune system than free-living domesticated cats.
- Housing treated and untreated cats together can lead to cross-contamination and affect culture results.
- Culture is less sensitive than PCR for the detection of chlamydial organisms – it is likely the azithromycin cats that were negative on culture remained persistently infected.
- Clinical scoring is subject to subjective bias, though this was reduced by blinding the investigator to the treatment group.
- Dosage and dosing regime for azithromycin is poorly characterised in cats and the regime used in this study may have negatively affected the results
|
Dean (2005)
| Population: |
Pathogen-free experimental colony cats aged 5-6 months. |
| Sample size: |
15 (13 entire females, 2 entire males). |
| Intervention details: |
- Inoculated with field strain of C. felis via the cornea.
- 7 days post-infection all cats were showing clinical signs and randomly assigned to one of three groups:
- 4 cats untreated
- 6 cats doxycycline 10mg/kg PO q24h for 7 days
- 5 cats doxycycline 10mg/kg PO q24h for 14 days
- If treatment was ineffective at eliminating infection (continued/ recurrence of clinical signs, or PCR-positive), rescue treatment 21-day course doxycycline 10mg/kg PO q24h was initiated.
- Monitoring of response to treatment:
- PCR copy numbers from conjunctival swabs (objective).
- Clinical scoring of disease (subjective but investigator blinded to treatment group).
- Cats were housed in rooms according to treatment group.
- Monitored for 6 months post-trial for recurrence.
|
| Study design: |
Randomised, single-blinded controlled trial. |
| Outcome Studied: |
Assess efficacy of 7-day and 14-day doxycycline treatment courses on the treatment and elimination of C felis using real-time PCR to monitor course of infection and response to treatment. |
Main Findings
(relevant to PICO question): |
- Doxycycline treated groups:
- Rapid decrease in PCR copy numbers and clinical scores within 2 days of treatment and apparent clinical cure by the end of treatment.
- All cats showed recurrence of disease after treatment end: 7-day cats within 4-7 days and 14-day cats within 14-21 days.
- All cats underwent 21-day rescue treatment:
- 8/11 cleared the infection.
- 3/11 required second rescue treatment of 28 days. One of these cats was from the 7-day doxycycline group and two of these cats were from the 14-day doxycycline group.
- All cats showed no recurrence in the following 6 months since last treatment.
- Authors’ recommendation is a 28-day course of doxycycline at 10mg/kg PO q24h required for elimination.
|
| Limitations: |
- Small number of participants means statistical analysis could not be applied.
- Use of an untreated group is questionable given previous studies.
- Randomisation method for assigning treatment groups and housing is not detailed.
- Experimental colony cats, due to their husbandry, may possess a less robust immune system than free-living domesticated cats.
- Clinical scoring is subject to subjective bias, though this was reduced by blinding.
- PCR does not necessarily detect active infection as it can also pick up dead bacterial material.
- Authors’ recommendation is not fully supported by the results. It is based on 3 cats failing to clear the infection following a 21-day rescue treatment, and clearing the infection following a 28-day treatment course. However, issues of resistance and a difference in the disease (acute versus chronic) may have played a role in the lack of elimination in 3 cats undergoing 21-day treatment
- Reinfection from other cats, or fomites, rather than true recrudescence could be responsible for the recurrence of clinical disease – housing the cats separately would have avoided this possible confounder. This means that it cannot categorically be said that 7 or 14 day courses of treatment do not fully eliminate infection in some cats.
|
Gerhardt (2006)
| Population: |
Owned cats presented to University of Munich teaching hospital suffering with conjunctivitis. All were negative for FIV/FeLV, had not been pre-treated with antibacterial agents, and were not showing clinical signs of central nervous system or renal disease. |
| Sample size: |
25 cats. |
| Intervention details: |
- Randomly assigned to one of two treatment groups:
- 14 cats enrofloxacin 5mg/kg SQ q24h for 3 days then 15mg enrofloxacin q24h PO for 11 days
- 11 cats doxycycline 5mg/kg SQ q12h for 3 days then 5mg/kg PO q12h for 11 days
- All cats received bromhexine hydrochloride 0.5mg/kg PO q8h and terbutaline 0.03mg/kg PO q8h for 14 days
- All cats were examined on days 1, 5, 10 and 14.
- Monitoring of response to treatment:
- IFA (immunofluorescence) detection of C felis by conjunctival swabs (objective).
- Conjunctivitis scores (subjective).
- Modified Karnofsky quality of life scores (subjective).
|
| Study design: |
Randomised, non-blinded controlled trial. |
| Outcome Studied: |
Compare efficacy of enrofloxacin and doxycycline in the treatment of conjunctivitis and C felis infection in naturally infected cats, and investigate the pharmacokinetics of enrofloxacin. |
Main Findings
(relevant to PICO question): |
- Enrofloxacin group:
- Generally more rapid improvement in conjunctivitis scores, though similar total improvement in groups by trial end.
- Greater improvement in quality of life scores on average than doxycycline.
- Both groups showed reduced shedding of C felis but none eliminated the organism during the trial
|
| Limitations: |
- Small numbers make statistical analysis less useful.
- Title references treatment of cats with C felis but the hypothesis is treatment of conjunctivitis and C felis infection.
- No details of cats’ sex, age or weight.
- No details on randomisation procedure.
- Use of injectable doxycycline for 3 days before starting oral therapy is not common practice.
- No details as to whether cats were hospitalised during study or owners were involved in treatment – potential non-compliance.
- Only treated for 14 days with no follow-up.
- Only 15 cats were positive for C. felis – 9 in the enrofloxacin group and 6 in the doxycycline group. However all 25 cats including those not infected with C. felis were included in the results, and not censored.
- Modified Kanorfsky scoring for quality of life scores to track clinical improvement is not widely used or well established, and subject to operator bias – it was developed by one of the authors in a previous paper and is an adaption of a human cancer patient scoring system from 1948. No details regarding which clinician was involved in scoring.
- IFA is considered the least sensitive method of diagnosing C. felis, largely surpassed by culture or PCR.
- Concurrent use of bromhexine hydrochloride and terbutaline may have affected clinical progression of disease
- The discussion does not reference all relevant preceding papers regarding doxycycline use in cats with C felis.
- The recommendation to treat for 21 days with enrofloxacin is not supported by the results.
- Use of enrofloxacin as a first-line treatment in the treatment of C felis is not compliant with best antibiotic prescribing guidelines. Cats should have been tested for other infectious agents e.g. FHV-1 and FCV as cofounding agents
- No details on funding or conflicts of interest.
|
Hartmann (2008)
| Population: |
Cats presented to University of Munich teaching hospital showing signs of upper respiratory disease or conjunctivitis or both. All were >6months of age, negative for FIV/FeLV, had not been pre-treated with antibacterials in the last 6 weeks, were not showing clinical signs of liver or renal disease and were not pregnant or nursing. Cats were either client-owned (10), farm cats (11) or shelter cats (18), and were of estimated ages (<1year: 13; 1-4 years: 16; 5-8 years: 8; 8-12 years: 2). Duration of clinical signs was unknown for most cats. |
| Sample size: |
39 cats (21 female, 13 neutered; 18 male, 12 neutered). |
| Intervention details: |
- Cats randomly assigned to one of two groups:
- 17 cats pradofloxacin 5mg/kg PO q24h and placebo q12h
- 22 cats doxycycline 5mg/kg PO q12h and placebo q24h.
- Treatment for 42 days.
- Monitoring of response to treatment:
- PCR for C felis, FHV and Mycoplasma from conjunctival swabs PCR for FCV and Mycoplasma spp. from pharyngeal swabs (objective).
- Clinical scoring (subjective but investigators blinded to treatment group).
- Modified Kanorfsky quality of life score (subjective).
|
| Study design: |
Randomised, double-blinded controlled trial. |
| Outcome Studied: |
Investigate efficacy of pradofloxacin in the treatment of cats with clinical signs of upper respiratory tract disease and its ability to eliminate C felis and Mycoplasma infection in these cats. |
Main Findings
(relevant to PICO question): |
- Doxycycline group:
- 13/22 infected with C felis.
- All PCR negative and asymptomatic by trial end.
- 2/13 still PCR-positive by day 28, cleared by day 42.
- Pradofloxacin group:
- 10/17 infected with C felis.
- 4/10 (40%) PCR positive and showing clinical signs by trial end – 2 remained PCR positive throughout, 2 apparently cleared infection then recurred.
- Ineffective at predictably clearing C felis infections.
|
| Limitations: |
- Small numbers make statistical analysis less useful.
- No details on randomisation procedure.
- Apart from the 2 cats in the pradofloxacin group that remained PCR positive throughout, no indication which cats were hospitalised or treated at home, so compliance or chances of reinfection could not be assessed.
- No long-term follow up (trial stopped at 42 days).
- Rationale for 42 days’ treatment is a textbook reference.
- PCR is the most sensitive method of finding chlamydial DNA but does not differentiate between live and dead organisms.
- Clinical scoring subject to subjective bias.
- Modified Kanorfsky scoring for quality of life scores to track clinical improvement is not widely used or well established, and subject to operator bias.
- Use of pradofloxacin as a first-line treatment in the treatment of C felis is not compliant with best antibacterial prescribing guidelines.
- The recommendation to use pradofloxacin in young cats and those with liver disease as an alternative to doxycyline is not supported by the results. The implied contraindication in young cats is predicated on tooth discolouration which is infrequent and of no obvious clinical significance.
- Funded by Bayer Healthcare, who make a licensed pradofloxacin for cats and dogs.
|
Ploneczka-Janeczko (2008)
| Population: |
Privately-owned cats, aged 3-10 years, which had undergone doxycycline therapy and developed vomiting or diarrhoea within the first 3 days of treatment. |
| Sample size: |
14 cats (8 male, 6 female). |
| Intervention details: |
- Cats treated with roxithromycin 5mg/kg PO q12h for 28 days then had a treatment-free period of 28 days.
- Monitoring of response to treatment:
- PCR from conjunctival swabs (objective).
- Clinical scoring and weekly change in clinical signs (same/increased/decreased).
|
| Study design: |
Case series. |
| Outcome Studied: |
Evaluate the clinical efficacy of systemic roxithromycin in treating tetracycline-intolerant cats with chronic conjunctivitis caused by C felis. |
Main Findings
(relevant to PICO question): |
- All cats showed improvement in clinical scores with treatment.
- No cats cleared infection, and 9/14 showed increase in DNA copy numbers by end of the study (day 56).
|
| Limitations: |
- Case series with no controls.
- Rare to see C felis in cats of these ages, normally a disease of cats <12 months old so the possibility of co-morbidities is high.
- Cats were chronically infected – 8 cats had shown signs for >12months, 5 for 6-12 months and 1 for 3-6 months.
- PCR is the most sensitive method of finding chlamydial DNA but does not differentiate between live and dead organisms.
- Conjunctival samples only taken at beginning and end of trial, so difficult to ascertain if ever PCR-negative.
- Clinical scoring subject to subjective bias and a change determined by increase/decrease/same lacks sensitivity.
- Relied on owners for compliance.
|
Appraisal, application and reflection
In all of the studies presented, systemic doxycycline therapy shows consistent efficacy against C felis both in bringing about rapid clinical improvement (however measured) within the first week of treatment, and, when given for a sufficient time period, has the most evidence for permanently eliminating infection. It is this latter aspect that makes it currently the most useful therapy versus other compounds studied (co-amoxiclav, pradofloxacin, enrofloxacin, azithromycin, roxithromycin), which, whilst bringing about clinical improvement appear insufficiently consistent at clearing infection. This is especially pertinent for shelter or stray cats, where C felis is commonplace, and infectious diseases require effective and reliable treatment to prevent spread within the facility.
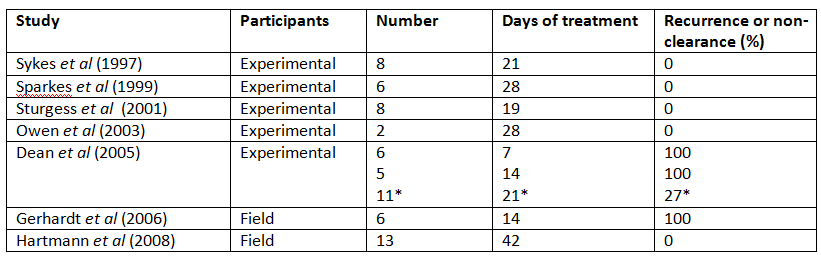
However, the question of how long a course of doxycycline needs to be is more difficult to answer from the studies available. The different course lengths can be summarised as follows:
The evidence available indicates that a 14-day course is insufficient, whilst a 21-day course may be sufficient in acute-stage infections which the experimental trials model. However, in field-infected cats, especially those in which the duration of infection is unknown, such as strays, a longer course may be indicated. In the study by Dean et al (2005), all the cats required rescue treatment after 7 or 14-day courses of treatment, and could therefore be considered chronically infected – in these, a 28-day course was required to eliminate infection from all cats (though 73% or 8/11 cleared the infection with a 21-day course). In shelters without finances to test for organism clearance, a 28-day course may be considered more appropriate; equally, in owned cats with acute infection, a 21-day course is likely to suffice. However, without more trials with greater participant numbers involving naturally infected cats, firm conclusions cannot be drawn.
By way of alternatives to doxycycline, co-amoxiclav has shown similar efficacy to doxycycline in improving clinical signs (Sturgess et al 2001) and pradofloxacin and enrofloxacin have shown a mildly better rate of clinical improvement (Gerhardt et al 2006; Hartmann et al 2008). However, only co-amoxiclav has been shown to consistently (that is, in all cats) clear infection, though a 30-day course was required for chronically infected cats, and a 19-day course given to acutely-infected cats that showed a high rate (62.5%) of recurrence (Sturgess et al 2001). Whilst doxycycline should remain the first-line treatment, co-amoxiclav, if given for a sufficient length of time (30 days), is a reasonable alternative.
One of the main weaknesses with the evidence presented here is the use of experimental cats, as their use limits extrapolation of results to field-infected free-living cats. Field infections may occur with greater doses of infectious agent, of different pathogenecity, in the face of multiple infections with other agents or against a background of other disease processes, in cats with greater genetic variation and on a variable nutritional plane. Therefore disease presentation, severity, and response to treatment may not match that seen in the field. For example, in stray or unowned animals, the chronicity of disease is unknown and response to treatment in these cases may be suboptimal, especially where secondary sequelae such as tear-duct scarring has occurred. Cats commonly present with C felis in addition to other pathogens of the upper respiratory tract disease complex (Hartmann et al 2010); secondary bacterial infection may complicate the clinical picture and delay resolution especially as tetracyclines appear to have only moderate efficacy against studied isolates (Schulz et al 2006). However, doxycycline has well-documented anti-inflammatory effects (e.g. Krakauer and Buckley 2003) which may help with improvement of clinical signs associated with viral co-infections
Several side-effects of oral doxycycline have been described. In a retrospective study of 168 cats, 13% developed vomiting, 11% diarrhoea, and 6% decreased appetite, and 36-40% showed increases in ALT or ALP during therapy (Schulz et al 2013). Oesophagitis, oesophageal stricture and tooth discolouration, whilst described elsewhere, (e.g. McGrotty and Knottenbelt 2002; German et al 2005) were absent. Gastrointestinal side effects may be attributable to the use of the doxycycline-hyclate salt which is acidic in solution, and is the compound present in the UK licensed veterinary agent (Ronaxan; Merial). Administration with food, or providing food or water after administration may reduce potential gastrointestinal side effects, whilst others (liver enzyme increase, tooth discolouration) appear clinically insignificant and do not represent valid reasons for not using the drug.
Methodology Section
| Search Strategy |
| Databases searched and dates covered: |
CAB Abstracts and PubMed from January 1973 to September 2016 |
| Search terms: |
(cat OR cats OR feline OR kitten) AND (chlamydia OR chlamydophila OR chlamydiosis OR chlamydophilosis OR psittaci) AND (treat* OR manag*) |
| Dates searches performed: |
3rd August and 4th September 2016 |
| Exclusion / Inclusion Criteria |
| Inclusion and exclusion criteria were defined before searching and are detailed below. |
| Exclusion: |
Review articles, single case reports, textbook chapters, conference proceedings. Papers not available in English or not accessible. Papers that described supportive treatment measures without concurrent antibiotic treatment assessment. Papers that described C felis infection in animals other than Felis catus. |
| Inclusion: |
Papers published between 1973 and present that evaluated the efficacy of antibiotic compounds for the treatment of clinical (experimental or natural) C felis infection in cats. Studies which had more than one aim, such as diagnostic modality investigation, were included. |
| Search Outcome |
|
Database
|
Number of results
|
Excluded – Review articles, single case reports etc.
|
Excluded – Not relevant to PICO
|
Excluded – Chlamydial studies in other species
|
Excluded – Not available in English or not accessible
|
Total relevant papers
|
|
CAB Direct
|
133 |
72 |
48 |
5 |
0 |
8 |
|
NCBI PubMed
|
54 |
8 |
17 |
21 |
0 |
7 |
|
Total relevant papers when duplicates removed
|
8 |
Conflict of Interest
The author declares no conflict of interest.
References
- Dean, R. et al. (2005) Use of Quantitative Real-time Pcr to Monitor the Response of Chlamydophila Felis Infection to Doxycycline Treatment. Journal of Clinical Microbiology, 43 (4), pp. 1858–1864. DOI: http://dx.doi.org/10.1128/JCM.43.4.1858-1864.2005
- Gerhardt, N. et al. (2006) Pharmacokinetics of Enrofloxacin and Its Efficacy in Comparison With Doxycycline in the Treatment of Chlamydophila Felis Infection in Cats With Conjunctivitis. Veterinary Record, 159 (18), PP. 591–594. DOI: http://dx.doi.org/10.1136/vr.159.18.591
- German, A. et al. (2005) Oesophageal Strictures in Cats Associated With Doxycycline Therapy. Journal of Feline Medicine and Surgery, 7 (1), PP. 33–41. DOI: http://dx.doi.org/10.1016/j.jfms.2004.04.001
- Hartmann, A. et al. (2010) Detection of Bacterial and Viral Organisms From the Conjunctiva of Cats With Conjunctivitis and Upper Respiratory Tract Disease. Journal of Feline Medicine and Surgery, 12 (10), pp. 775–82. DOI: http://dx.doi.org/10.1016/j.jfms.2010.06.001
- Hartmann, A. et al. (2008). Efficacy of Pradofloxacin in Cats With Feline Upper Respiratory Tract Disease Due to Chlamydophila Felis or Mycoplasma Infections. Journal of Veterinary Internal Medicine, 22, 44–52. DOI: http://dx.doi.org/10.1111/j.1939-1676.2007.0012.x
- Krakauer, T., Buckley, M. (2003). Doxycycline Is Anti-inflammatory and Inhibits Staphylococcal Exotoxin-induced Cytokines and Chemokines. Antimicrobial agents and chemotherapy, 47 (11), pp. 3630–3. DOI: http://dx.doi.org/10.1128/AAC.47.11.3630-3633.2003
- McGrotty, Y. and Knottenbelt, C. (2002) Oesophageal Stricture in a Cat Due to Oral Administration of Tetracyclines. The Journal of Small Animal Practice, 43 (5), pp. 221–3. http://dx.doi.org/10.1111/j.1748-5827.2002.tb00062.x
- Owen, W. et al. (2003) Efficacy of Azithromycin for the Treatment of Feline Chlamydophilosis. Journal of Feline Medicine and Surgery, 5(6), 305–11. DOI: http://dx.doi.org/10.1016/S1098-612X(03)00072-X
- Ploneczka-Janeczko, K. et al. (2015) Reduction of Chlamydophila-felis-associated Signs by Roxithromycin Treatment Regimen in Cats Showing Doxycycline Intolerance. Veterinarni Medicina, 60 (11), PP. 654–661. DOI: http://dx.doi.org/10.17221/8534-VETMED
- Schulz, B. Wolf, G. and Hartmann, K. (2006) Bacteriological and Antibiotic Sensitivity Test Results in 271 Cats With Respiratory Tract Infections. Veterinary Record, 158, pp. 269-270. DOI: http://dx.doi.org/10.1136/vr.158.8.269
- Schulz, B. et al. (2013) Side Effects Suspected to Be Related to Doxycycline Use in Cats. Veterinary Record, 172, pp. 184–185. DOI: http://dx.doi.org/10.1136/vr.101031
- Sparkes, A. et al. (1999) The Clinical Efficacy of Topical and Systemic Therapy for the Treatment of Feline Ocular Chlamydiosis. Journal of Feline Medicine and Surgery, 1 (1), pp. 31–35. DOI: http://dx.doi.org/10.1016/S1098-612X(99)90007-4
- Sturgess, C. (2001) Controlled Study of the Efficacy of Clavulanic Acid-potentiated Amoxycillin in the Treatment of Chlamydia Psittaci in Cats. Veterinary Record, 149, pp. 73–76. DOI: http://dx.doi.org/10.1136/vr.149.3.73
- Sykes, J. (1999) Comparison of the Polymerase Chain Reaction and Culture for the Detection of Feline Chlamydia Psittaci in Untreated and Doxycycline-treated Experimentally Infected Cats. Journal of Veterinary Internal Medicine, 13, pp. 146–52. DOI: http://dx.doi.org/10.1111/j.1939-1676.1999.tb02171
Intellectual Property Rights
Knowledge Summaries are a peer-reviewed article type which aims to answer a clinical question based on the best available current evidence. It does not override the responsibility of the practitioner. Informed decisions should be made by considering such factors as individual clinical expertise and judgement along with patient’s circumstances and owners’ values. Knowledge Summaries are a resource to help inform and any opinions expressed within the Knowledge Summaries are the author's own and do not necessarily reflect the view of the RCVS Knowledge.
Authors of Knowledge Summaries submitted to RCVS Knowledge for publication will retain copyright in their work, but will be required to grant to RCVS Knowledge an exclusive licence of the rights of copyright in the materials including but not limited to the right to publish, re-publish, transmit, sell, distribute and otherwise use the materials in all languages and all media throughout the world, and to licence or permit others to do so.
Authors will be required to complete a licence for publication form, and will in return retain certain rights as detailed on the form.